Surgery for Secondary Liver Cancer
Liver Resection
There is strong evidence that selected patients with secondary liver cancer amenable to surgery may be offered worthwhile palliation and possible cure. There are numerous published studies from all over the world where it has been shown that 25% - 38% of patients achieved a 5 year survival after successful surgery for secondary liver cancer. Currently fewer than a third of suitable patients are being offered liver surgery.
Major surgery on the liver which is a large soft organ with an enormous blood supply, may now be performed safely with a low complication rate. There is now a much better understanding of the segmental anatomy of the liver. The CUSA (Cavitron Ultrasonic Surgical Aspirator), an instrument designed for neurosurgery (brain surgery), is useful in liver surgery. Its tip selectively fragments liver cells leaving blood vessels and bile ducts exposed. Blood vessels are not fragmented as they are made of firmer fibrous tissue. Once exposed they are then divided, thus avoiding any significant blood loss which means that it is safe to remove individual segments, one half or even 70% of a liver. The remaining liver substance increases rapidly in size as the liver has enormous powers of regeneration.
There is evidence to show that liver surgery is safe and can be carried out with relatively few complications provided that it is carried out by a trained liver surgeon. Liver surgery may be carried out with a low operative mortality. It is less than 2% in our Unit. Surgeons offering liver resection should be able to offer similar mortality rates. In addition it has been shown that transfusion rates can be kept to a minimum - 5% in our Unit.
Although survival rates of up to 40% at 5 years have been published, we have shown that it is possible by combining chemotherapy with surgery to achieve 50% survival at 5 years.
It has become apparent that patients with extensive liver disease may have their disease controlled and reduced in extent by the use of pre-operative chemotherapy. Patients with inoperable liver cancer may find that their liver disease becomes operable after preliminary treatment with neo-adjuvant chemotherapy. The results of surgery in this group of patients confirms that 35% could survive 5 years after such an approach.
There are many reasons why patients are not offered surgery. In some cases this stems from lack of knowledge whilst in others individual prejudices play a part. Even today a lot of doctors simply do not realise that modern liver surgery is completely safe in the hands of an experienced liver surgeon. Despite numerous series in the literature doctors may be unaware of the survival advantage that successful resection may confer - some simply refuse to accept what is already published.
Sadly many patients who are potentially operable are not referred for an opinion and such patients may miss out on the only prospect of prolonging their lives or even being cured.
Techniques to Improve Resection Rates
Staged liver resection
Here an anatomical liver resection is performed removing the bulk of the disease. After 6 weeks when compensatory hypertrophy has occurred a further liver operation may be performed to remove the residual disease from the remaining liver.
Pre-operative Portal Vein Embolisation
In patients where an anatomical liver resection may not leave the patient with an adequate volume of residual liver Pre-Operative Portal Vein embolisation (PVE) of the side to be removed will lead to compensatory hypertrophy of the portion of liver to be preserved over a period of 4 to 6 weeks. Thus by the time the surgery is done the residual liver is already much enlarged thus reducing the risk of insufficiency of the liver.
 |
 |
1 - Figure 1 - two right sided colonic Secondaries in a young patient with a small left liver. Proposed resection line marked with arrow. Removal of the right liver (area to the left of arrow on scan) would leave this patient at risk of liver insufficiency. |
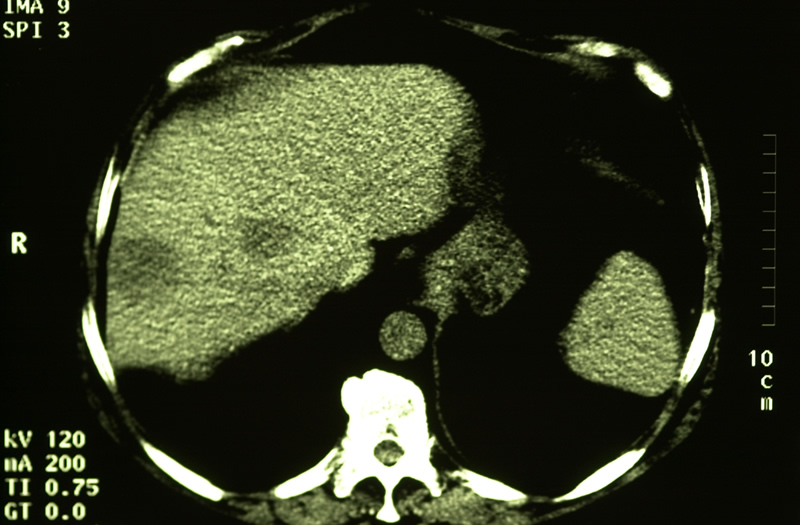
Figure 1 - click image to enlarge |
|
|
2 - Figure 2 - the portal vein is canulated via the left liver and the catheter passed into the right portal vein. |
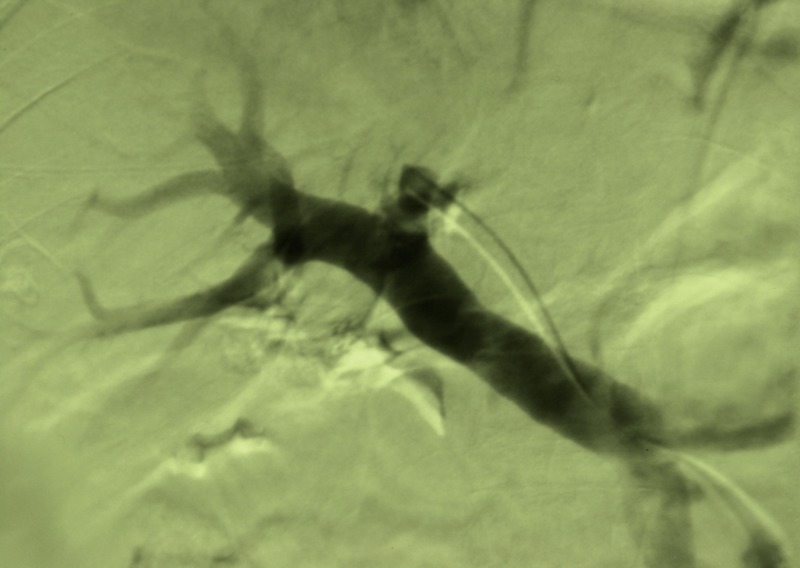
Figure 2 - click image to enlarge |
|
|
| 3 - Figure 3 - successful right portal vein embolisation was followed by compensatory enlargement of the left liver over 4 weeks and this patient tolerated a resection of the right liver extended to include segment 4A of the left liver. |
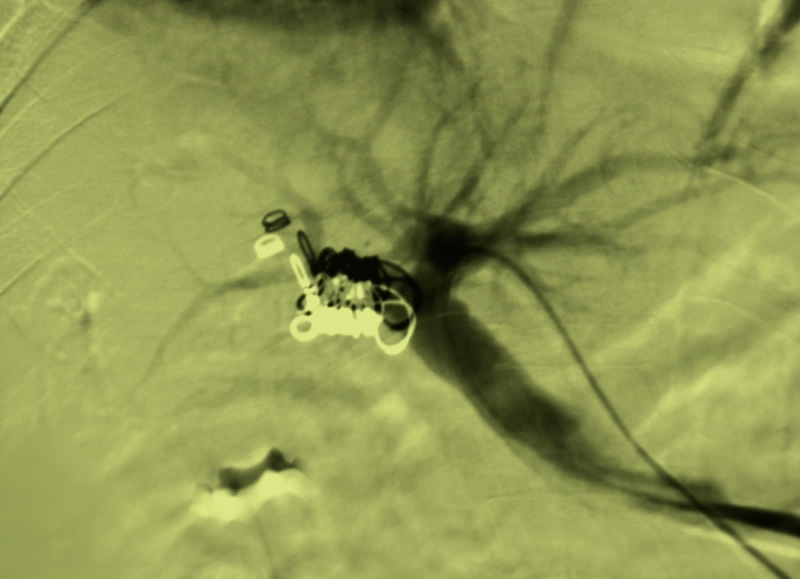
Figure 2 - click image to enlarge |